
Joint pain is usually treated as a joint problem. Rest it. Ice it. Take something for the inflammation. Repeat.
But a growing body of research is pointing to a different origin story — one that begins not in the knee or the hip or the shoulder, but in the gut. The connection between the two is now well enough established that researchers have given it a name: the gut-joint axis. And understanding it may fundamentally change how we think about joint pain, particularly the kind that seems to appear from nowhere.
Table Of Contents:
The Gut-Joint Axis: A Highway You Didn't Know Existed
Your gut and your joints are in constant conversation.
Not metaphorically. Through the bloodstream, through the immune system, through the thousands of compounds your gut bacteria produce every hour of every day, your intestinal ecosystem is continuously sending signals that reach your joint tissue. When those signals are anti-inflammatory, your joints are protected. When they are not, something very different begins to happen.
Researchers now call this the gut-joint axis. And the more they study it, the more significant it appears to be.
The basic mechanism works like this. Your gut bacteria produce a vast array of compounds — short-chain fatty acids, enzymes, metabolites — that enter systemic circulation and travel throughout the body. In a healthy, diverse microbiome, these compounds tend to be anti-inflammatory and tissue-protective. In a disrupted microbiome, they tend to be the opposite. The joints, it turns out, are one of the places where this difference shows up most clearly.
But the research goes further than that — and this is where it gets genuinely surprising.
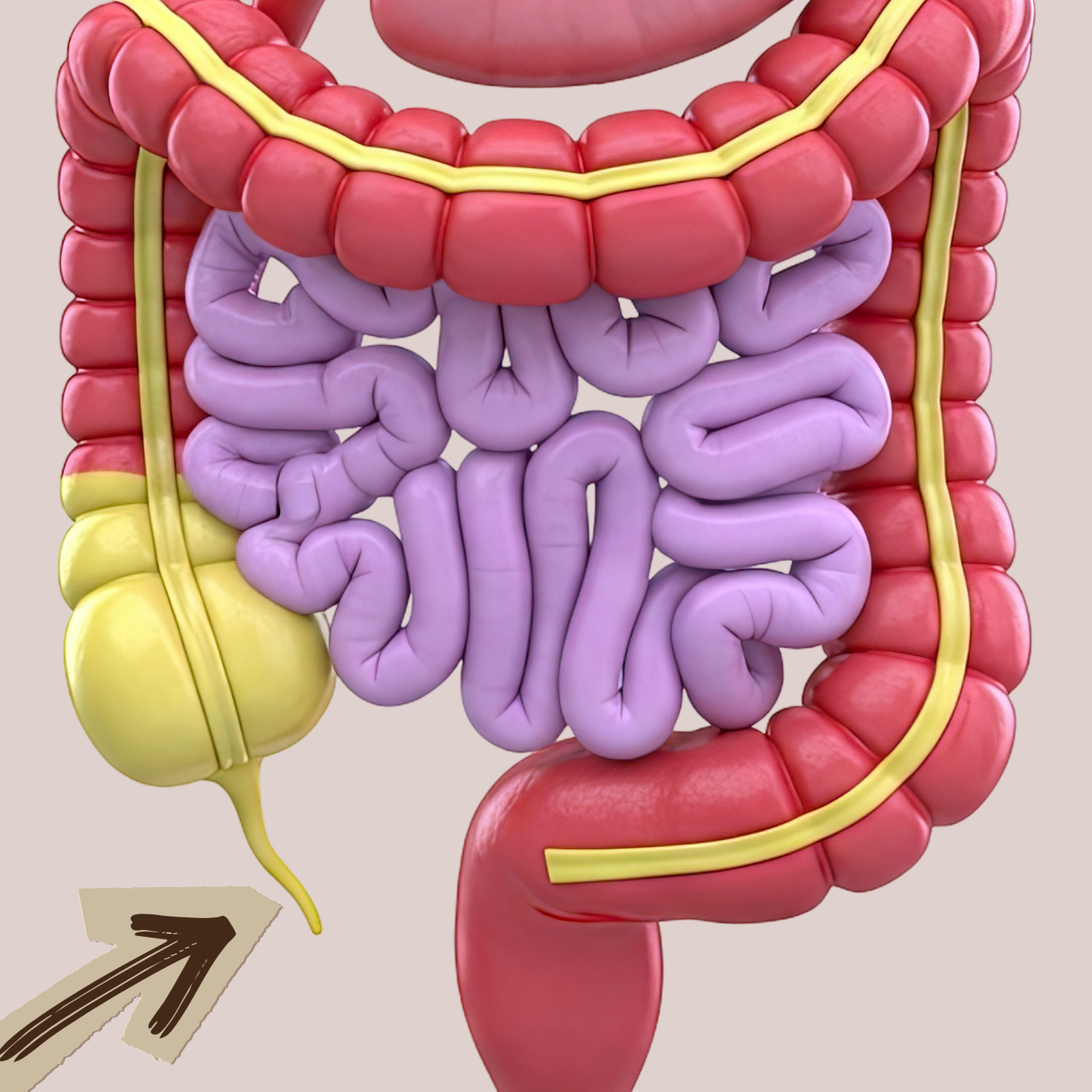
Scientists have found bacterial DNA from species including Prevotella, Fusobacterium, and Bacteroides inside synovial fluid — the liquid that cushions and lubricates your joints. Not in the gut. In the joints. This suggests the gut-joint connection is not just a distant, systemic one. Microbial material may actually be travelling to joint tissue and triggering immune activation right there, inside the joint itself.
One species keeps appearing with particular consistency. Prevotella copri has been identified at elevated levels in rheumatoid arthritis patients across multiple studies — and crucially, not just in people who already have symptoms. It shows up in the preclinical stages of the disease, before joint symptoms have fully developed. In other words, the microbial disruption appears to come first.
That is not a marginal finding. It is a significant one. It means the question worth asking may no longer be "what is wrong with my joints?" but "what is happening in my gut?"
Leaky Gut: The Missing Link
Running the entire length of your digestive tract is a barrier so thin it is only one cell thick. This lining — your intestinal barrier — is one of the most important structures in your body, and most people have never heard of it.
Its job is to act as a highly selective gatekeeper. Held together by proteins called tight junctions, it decides what crosses from your gut into your bloodstream and what doesn't. Nutrients in. Harmful compounds out. When it is working properly, this system is extraordinarily precise.
When it breaks down, the consequences ripple through the entire body.
A compromised intestinal barrier — what researchers call increased intestinal permeability, and what most people now call leaky gut — allows fragments of bacteria to slip through into the bloodstream. These fragments, called lipopolysaccharides or LPS, come from the outer membranes of harmful gut bacteria. They are intensely pro-inflammatory. And once they are in circulation, the immune system responds to them as a threat — triggering a systemic inflammatory response that travels to tissues throughout the body.
Including the joints.

Research has now found LPS and LPS-binding proteins inside the synovial fluid of osteoarthritis patients — the fluid that should be cushioning and protecting the joint. Their presence there is associated with activated macrophages, worsening joint space narrowing, more severe bone spurs, and higher pain scores. The inflammatory signal that started in a damaged gut lining is ending up inside the joint itself.
This may explain something that frustrates a lot of people: joint pain with no clear structural cause. No injury. No diagnosis that fully accounts for it. Just persistent aching and stiffness that seems to have appeared from nowhere. If the gut barrier is compromised and LPS is circulating, joint inflammation can occur without any mechanical trigger at all.
There is a second, quieter mechanism running alongside this one.
When the gut microbiome is disrupted, populations of butyrate-producing bacteria decline. Butyrate is a short-chain fatty acid made when beneficial bacteria ferment dietary fiber — and it is one of the most powerful anti-inflammatory compounds the gut produces. Among its many roles, butyrate directly suppresses the inflammatory enzymes responsible for degrading cartilage. When butyrate-producing bacteria are depleted, that protection disappears. The inflammatory enzymes go unchecked. Cartilage breaks down faster.
Two mechanisms, both originating in the gut. Both arriving, eventually, in the joints.
Inflammaging: Why It Gets Worse in Midlife
If joint pain seemed to appear out of nowhere in your forties, fifties, or sixties — you are not imagining it. And it is not simply a matter of getting older.
It coincides with something very specific happening in the gut.
Researchers have identified a phenomenon they call inflammaging — a chronic, low-grade inflammatory state that builds gradually as the microbiome loses diversity and protective function with age. It is not dramatic. It does not announce itself. It accumulates quietly, over years, until the inflammatory load crosses a threshold that the body can no longer absorb silently.
The microbial shift that drives it is consistent and well-documented. With age, populations of butyrate-producing, anti-inflammatory bacteria progressively decline. Biodiversity falls. And in their place, bacteria associated with inflammation and disease begin to take a larger share of the ecosystem.
Faecalibacterium prausnitzii is among the most important of these declining bacteria. It is one of the most abundant anti-inflammatory species in a healthy human gut, and its reduction has been associated with elevated inflammatory markers and a range of chronic inflammatory conditions. As populations of bacteria like this one shrink, the balance tips — from a microbiome that dampens inflammation to one that amplifies it.
For women, this shift is compounded by menopause in ways that make the timing of joint pain even less coincidental. Oestrogen plays a significant and underappreciated role in maintaining microbial diversity. As oestrogen declines through perimenopause and beyond, so does the diversity of the gut microbiome that keeps inflammation in check. Research has found that postmenopausal women have measurably less diverse gut microbiomes than premenopausal women, with lower levels of key anti-inflammatory species including Akkermansia muciniphila.
The result is a perfect storm: a less resilient gut barrier, less butyrate production, higher circulating LPS, and more systemic inflammation reaching the joints. Not one cause, but several — all pointing in the same direction at the same time.
And then there is the factor that almost nobody talks about.
The medications most commonly used to manage joint pain — ibuprofen, naproxen, diclofenac, the NSAIDs — may be aggravating the very problem they are treating. These drugs provide real short-term relief by blocking inflammatory enzymes. But research now shows they also damage the intestinal lining, widening the tight junctions that hold the gut barrier together and increasing the permeability that allows LPS to enter the bloodstream.
In other words, they address the symptom while worsening one of the root causes — and the cycle quietly feeds itself. More pain leads to more NSAIDs. More NSAIDs means more gut barrier damage. More gut barrier damage means more inflammation reaching the joints.
This does not mean NSAIDs should never be used. There are times when they are appropriate and necessary. But for people who rely on them regularly over years, this cycle may explain why things may not be improving the way they should.

What You Can Actually Do About It
Understanding the gut-joint axis is only useful if it changes something. And the good news is that it does — because the microbiome is not fixed. It is responsive, and diet is the most powerful lever we have for shifting its composition.
Feed your protective bacteria first. Prebiotic fiber is the foundation of everything else. Without it, beneficial bacteria cannot thrive, butyrate production falls, and the inflammatory cascade begins. Garlic, onions, leeks, asparagus, oats, legumes, and resistant starch (found in cooled cooked potatoes and rice) are all excellent sources. The goal is not just more fiber but more variety as different fibers feed different species. The Bifidobacterium and Faecalibacterium populations that decline with age are particularly dependent on inulin and fructooligosaccharides — found in abundance in the foods listed above.
Add polyphenols to every meal. Berries, extra virgin olive oil, green tea, dark chocolate, and deeply coloured vegetables all contain polyphenols that feed anti-inflammatory gut bacteria while suppressing the harmful ones. They also help seal the gut barrier — directly addressing the leaky gut mechanism that allows LPS into the bloodstream.
Eat fermented foods regularly. Foods like kefir, sauerkraut, kimchi, and kombucha introduce live bacteria directly into the gut. A landmark Stanford study found that a high-fermented-food diet increased microbiome diversity and reduced 19 inflammatory proteins — including the cytokines that drive chronic joint inflammation. Even small daily amounts appear to make a meaningful difference over time.
Get consistent omega-3s. Ground flaxseed, chia seeds, walnuts, and hemp seeds provide plant-based omega-3 fatty acids that do two things relevant to joints: they support the structural integrity of the gut barrier and they directly reduce the inflammatory prostaglandins that drive joint pain.

Consider targeted probiotic support. A 2025 meta-analysis of randomised controlled trials found that probiotic supplementation significantly reduced osteoarthritis severity scores and improved physical function in knee osteoarthritis patients. Lactobacillus casei and Lactobacillus acidophilus are among the most studied strains for joint inflammation, with clinical trials showing reductions in key inflammatory markers.
Don't overlook the structural nutrients. The microbiome creates the conditions for joint health, but specific nutrients do the repair work. Vitamin D regulates immune responses and is frequently deficient in people with inflammatory joint conditions. Magnesium supports hundreds of enzymatic processes central to cartilage metabolism and is chronically low in a large proportion of adults. Calcium and vitamin K2 work together to direct calcium into bones and joints rather than soft tissue — K2 is the often-missing piece that makes calcium supplementation actually useful. Collagen synthesis requires vitamin C, zinc, and glycine. And critically, the microbiome directly influences how well all of these nutrients are absorbed — which means gut health and nutritional status are inseparable.
Remove the obvious obstacles. Ultra-processed foods, refined sugar, and excess alcohol all actively promote the growth of pro-inflammatory bacteria, damage the gut lining, and feed the systemic inflammation that reaches the joints. No amount of prebiotic fiber can fully compensate for a diet that is simultaneously dismantling the ecosystem it is trying to build.
Add in some remedies. Two natural compounds have strong enough evidence for joint inflammation to be worth adding to the dietary strategies above. Turmeric — curcumin specifically — has been studied head-to-head against prescription anti-inflammatory drugs with comparable results, blocking the same inflammatory pathways as ibuprofen but without any of the gut damage. Boswellia works through a completely different pathway, targeting an enzyme system that most anti-inflammatory drugs don't even touch. In one study, patients who stopped taking Boswellia kept their improvements for a full month afterwards — while those who stopped the prescription drug lost their benefits almost immediately. Together, these two compounds cover more inflammatory ground than either one alone, and both protect the gut barrier rather than erode it.
The Bottom Line
Joint pain in midlife is not inevitable. And it is not simply a mechanical problem that you manage with painkillers and hope for the best.
The gut-joint axis gives us something genuinely different: a new way of understanding where the pain is coming from — and a new set of levers for addressing it. Dysbiosis allows pro-inflammatory compounds to leak into the bloodstream. A declining microbiome strips away the butyrate that protects cartilage. The medications most commonly used to manage the pain quietly worsen the gut dysfunction driving it. And in women, the microbiome shifts that accompany menopause accelerate everything.
None of that is inevitable either.
The microbiome is not fixed. It is one of the most responsive systems in the human body — and diet is the most powerful tool we have for changing it. The changes can begin within days of shifting what you eat. The right bacteria can be nourished back. The gut barrier can be strengthened. The inflammatory signals reaching your joints can be reduced.
Every meal is either feeding the bacteria that protect your joints or the ones that inflame them. That is not a small thing. It is, in fact, exactly where to start.




What Do You Think? Comment Below: